
15 Childbirth
Onset of Labor
Childbirth typically occurs within a week of a woman’s due date, unless the woman is pregnant with more than one fetus, which usually causes her to go into labor early. As a pregnancy progresses into its final weeks, several physiological changes occur in response to hormones that trigger labor.
A common sign that labor is beginning is the so-called “bloody show.” During pregnancy, a plug of mucus accumulates in the cervical canal, blocking the entrance to the uterus. Approximately 1–2 days prior to the onset of true labor, this plug loosens and is expelled, along with a small amount of blood.
As labor nears, the mothers’ pituitary gland produces oxytocin. This begins to stimulate stronger, more painful uterine contractions, which—in a positive feedback loop—stimulate the secretion of prostaglandins from fetal membranes. Like oxytocin, prostaglandins also enhance uterine contractile strength. The fetal pituitary gland also secretes oxytocin, which increases prostaglandins even further.
And the stretching of the cervix by a full-term fetus in the head-down position is regarded as a stimulant to uterine contractions. Combined, these stimulate true labor.[1]
Stages of Birth for Vaginal Delivery
https://youtube.com/watch?v=samWyTjFmS8%3Fsi%3D7EsV9ce9thtlihWY
Video offers a brief introduction of the three stages of vaginal delivery
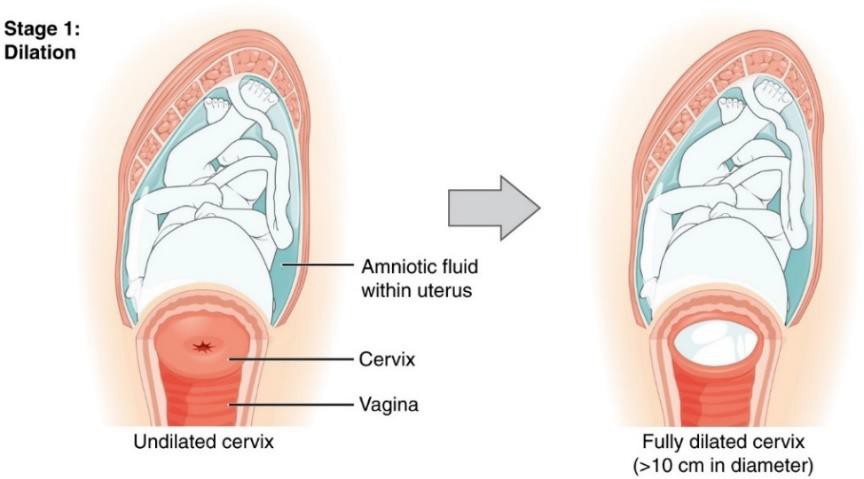
The First Stage
Uterine contractions signify that the first stage of labor has begun. These contractions may initially last about 30 seconds and be spaced 15 to 20 minutes apart. These increase in duration and frequency to more than a minute in length and about 3 to 4 minutes apart. Typically, doctors advise that they be called when contractions are coming about every 5 minutes. Some women experience false labor or Braxton-Hicks Contractions, especially with the first child.
These may come and go. They tend to diminish when the mother begins walking around. Real labor pains tend to increase with walking. In one out of 8 pregnancies, the amniotic sac or water in which the fetus is suspended may break before labor begins. In such cases, the physician may induce labor with the use of medication if it does not begin on its own in order to reduce the risk of infection. Normally this sac does not rupture until the later stages of labor.
The first stage of labor is typically the longest. During this stage the cervix or opening to the uterus dilates to 10 centimeters or just under 4 inches. This may take around 12-16 hours for first children or about 6-9 hours for women who have previously given birth. Labor may also begin with a discharge of blood or amniotic fluid.
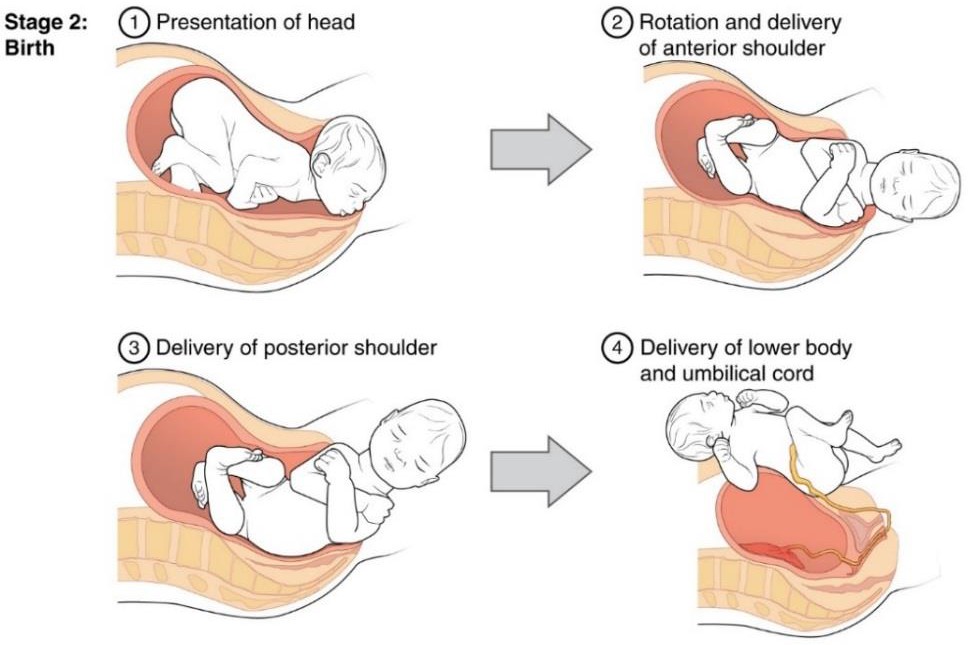
The Second Stage
The passage of the baby through the birth canal is the second stage of labor. This stage takes about 10-40 minutes. Contractions usually come about every 2-3 minutes. The mother pushes and relaxes as directed by the medical staff. Normally the head is delivered first. The baby is then rotated so that one shoulder can come through and then the other shoulder. The rest of the baby quickly passes through. At this stage, an episiotomy, or incision made in the tissue between the vaginal opening and anus, may be performed to avoid tearing the tissue of the back of the vaginal opening (Mayo Clinic, 2016). The baby’s mouth and nose are suctioned out. The umbilical cord is clamped and cut.
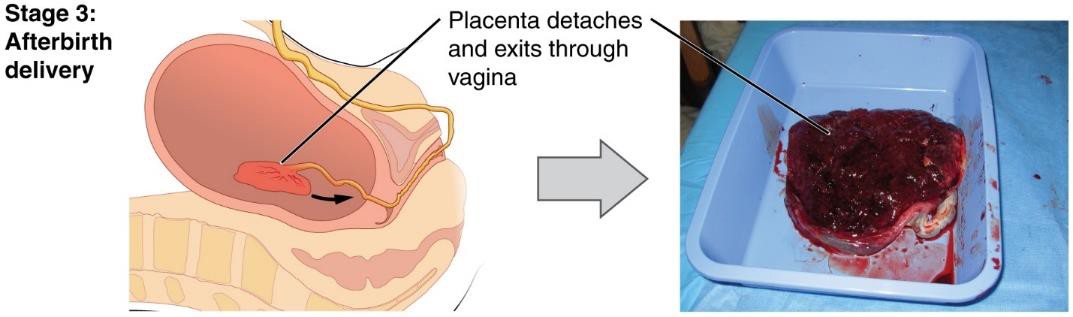
The Third Stage
The third and final stage of labor is relatively painless. During this stage, the placenta or afterbirth is delivered. This is typically within 20 minutes after delivery. If an episiotomy was performed it is stitched up during this stage.
Additional Considerations
More than 50% of women giving birth at hospitals use an epidural anesthesia during delivery (American Pregnancy Association, 2015). An epidural block is a regional analgesic that can be used during labor and alleviates most pain in the lower body without slowing labor. The epidural block can be used throughout labor and has little to no effect on the baby. Medication is injected into a small space outside the spinal cord in the lower back. It takes 10 to 20 minutes for the medication to take effect. An epidural block with stronger medications, such as anesthetics, can be used shortly before a Cesarean Section or if a vaginal birth requires the use of forceps or vacuum extraction.
Women giving birth can also receive other pain medications (although medications given through injection can have negative side effects on the baby). In emergency situations (such as the need for a C-section), women may be given general anesthesia. They can also choose not to utilize any pain medications. That is often referred to as natural childbirth.

Women can also use alternate positions (including standing, squatting, being on hands and knees, and using a birthing stool) and laboring, and even delivering in tubs of warm water to help relieve the pain of childbirth.
Video offers a more detailed introduction to the three stages of vaginal delivery.
Medical Interventions in Childbirth
Sometimes women cannot go into labor on their own and/or deliver vaginally. Let’s look at induction of labor and Cesarean Sections.
Sometimes a baby’s arrival may need to be induced before labor begins naturally. Induction of labor may be recommended for a variety of reasons when there is concern for the health of the mother or baby. For example:
- The mother is approaching two weeks beyond her due date and labor has not started naturally
- The mother’s water has broken, but contractions have not begun
- There is an infection in the mother’s uterus
- The baby has stopped growing at the expected pace
- There is not enough amniotic fluid surrounding the baby
- The placenta peels away, either partially or completely, from the inner wall of the uterus before delivery
- The mother has a medical condition that might put her or her baby at risk, such as high blood pressure or diabetes (Mayo Clinic, 2014).
A Cesarean Section (C-section) is surgery to deliver the baby by being removed through the mother’s abdomen. In the United States, about one in three women have their babies delivered this way (Martin et al., 2015). Most C-sections are done when problems occur during delivery unexpectedly. These can include:
- Health problems in the mother
- Signs of distress in the baby
- Not enough room for the baby to go through the vagina
- The position of the baby, such as a breech presentation where the head is not in the downward position.
 |
 |
C-sections are also more common among women carrying more than one baby. Although the surgery is relatively safe for mother and baby, it is considered major surgery and carries health risks. Additionally, it also takes longer to recover from a C-section than from vaginal birth. After healing, the incision may leave a weak spot in the wall of the uterus. This could cause problems with an attempted vaginal birth later. In the past, doctors were hesitant to allow a vaginal birth after a C-section. However, now more than half of women who have a C-section go on to have a vaginal birth later.[2] This is referred to as a Vaginal Birth After Cesarean (VBAC).[3]
- 28.4 Maternal Changes During Pregnancy, Labor, and Birth by Lindsay M. Biga, Sierra Dawson, Amy Harwell, Robin Hopkins, Joel Kaufmann, Mike LeMaster, Philip Matern, Katie Morrison-Graham, Devon Quick, and Jon Runyeon is licensed under CC BY-NC-SA 4.0 ↵
- Lifespan Development: A Psychological Perspective by Martha Lally and Suzanne Valentine-French is licensed under CC BY-NC-SA 3.0 ↵
- Child Growth and Development by Jennifer Paris, Antoinette Ricardo, & Dawn Rymond licensed under CC BY 4.0 ↵
