
26 Health
Infants depend on the adults that care for them to promote and protect their health. The following section addresses common physical conditions that can affect infants, the danger of shaking babies, and the importance of immunizations.
Common Physical Conditions and Issues during Infancy
Some physical conditions and issues are very common during infancy. Many are normal, and the infant’s caregivers can deal with them if they occur. Mostly, it is a matter of the caregivers learning about what is normal for their infant and getting comfortable with the new routine in the household. New parents and caregivers often have questions about the following:
Bowel Movements
Infants’ bowel movements go through many changes in color and consistency, even within the first few days after birth. While the color, consistency, and frequency of stool will vary, hard or dry stools may indicate dehydration and increased frequency of watery stools may indicate diarrhea.

Colic
Many infants are fussy in the evenings, but if the crying does not stop and gets worse throughout the day or night, it may be caused by colic. According to the American Academy of Pediatrics, about one-fifth of all infants develop colic, usually starting between 2 and 4 weeks of age. They may cry inconsolably or scream, extend or pull up their legs, and pass gas. Their stomachs may be enlarged. The crying spells can occur anytime, although they often get worse in the early evening.
The colic will likely improve or disappear by the age of 3 or 4 months. There is no definite explanation for why some infants get colic. Health care providers can help ensure there is no medical reason behind the crying.
Some infants seem to be soothed by being held, rocked, or wrapped snugly in a blanket. Some like a pacifier.[1]

Shaken Baby Syndrome
Here is a PSA from the Center for Disease Control (CDC)
The crying.
The late-night feedings. The diaper changes.
The exhaustion
If you’ve ever been around a baby who won’t stop crying, you know there’s potential to get frustrated. Focus on calming yourself and understand that you may not be able to calm your baby. It’s not your fault or your baby’s.[2]
It’s normal for healthy babies to cry and some babies cry much more than others. And they cannot always be consoled and caregivers can feel pushed to the limit. When caregivers lose control and shake a baby it can have devastating effects.
Shaken Baby Syndrome (SBS) is a severe form of physical child abuse. SBS may be caused from vigorously shaking an infant by the shoulders, arms, or legs. The “whiplash” effect can cause intracranial (within the brain) or intraocular (within the eyes) bleeding. Often there is no obvious external head trauma. Still, children with SBS may display some outward signs:
- Change in sleeping pattern or inability to be awakened
- Confused, restless, or agitated state
- Convulsions or seizures
- Loss of energy or motivation
- Slurred speech
- Uncontrollable crying
- Inability to be consoled
- Inability to nurse or eat
SBS can result in death, cognitive and developmental delays, paralysis, severe motor dysfunction, spasticity, blindness, and seizures.
Who’s at Risk?
Small children are especially vulnerable to this type of abuse. Their heads are large in comparison to their bodies, and their neck muscles are weak. Children under one year of age are at highest risk, but SBS has been reported in children up to five years of age. Shaking often occurs in response to a baby crying or having a toilet-training accident. The perpetrator tends to be male and is primarily the biological father or the mother’s boyfriend or partner. Caregivers are responsible for about 9%-21% of cases. The explanation typically provided by the caregiver—”I was playing with the baby”—does not begin to account for the severity of trauma. Many times there is also a history of child abuse.
Can It Be Prevented?
SBS is completely preventable. However, it is not known whether educational efforts will effectively prevent this type of abuse. Home visitation programs are shown to prevent child abuse in general. Because the child’s father or the mother’s partner often causes SBS, they should be included in home visitation programs. Home visits bring community resources to families in their homes. Health professionals provide information, healthcare, psychological support, and other services that can help people to be more effective parents and caregivers.
The Bottom Line
- Shaking a baby can cause death or permanent brain damage. It can result in life-long disability.
- Healthy strategies for dealing with a crying baby include:
- finding the reason for the crying
- checking for signs of illness or discomfort, such as diaper rash, teething, tight clothing;
- feeding or burping;
- soothing the baby by rubbing its back; gently rocking; offering a pacifier; singing or talking;
- taking a walk using a stroller or a drive in a properly-secured car seat;
- or calling the doctor if sickness is suspected
- All babies cry. Caregivers often feel overwhelmed by a crying baby. Calling a friend, relative, or neighbor for support or assistance lets the caregiver take a break from the situation. If immediate support is not available, the caregiver could place the baby in a crib (making sure the baby is safe), close the door, and check on the baby every five minutes.[3]

Abusive Head Trauma
Shaken baby syndrome is part abusive head trauma (AHT), severe form of physical child abuse that results in an injury to the brain of a child. This is important to note because:
- Abusive head trauma is a leading cause of physical child abuse deaths in children under 5 in the United States.
- Abusive head trauma accounts for approximately one third of all child maltreatment deaths.
- The most common trigger for abusive head trauma is inconsolable crying.
- Babies less than one year old are at greatest risk of injury from abusive head trauma.[4]
Teething
Although newborns usually have no visible teeth, baby teeth begin to appear generally about 6 months after birth. During the first few years, all 20 baby teeth will push through the gums, and most children will have their full set of these teeth in place by age 3.
An infant’s front four teeth usually appear first, at about 6 months of age, although some children don’t get their first tooth until 12-14 months. As their teeth break through the gums, some infants become fussy, and irritable; lose their appetite; or drool more than usual.
The FDA does not recommend gum-numbing medications with an ingredient called benzocaine because they can cause a potentially fatal condition in young children. Safe forms of relief include a chilled teething ring or gently rubbing the child’s gums with a clean finger.
Spitting Up/Vomiting
Spitting up is a common occurrence for young infants and is usually not a sign of a more serious problem. But if an infant is not gaining weight or shows other signs of illness, a health care provider should be consulted.

Urination
Infants urinate as often as every 1 to 3 hours or as infrequently as every 4 to 6 hours. In case of sickness or if the weather is very hot, urine output might drop by half and still be normal. If an infant shows any signs of distress while urinating or if any blood is found in a wet diaper medical care should be sought.
Diaper Rash
A rash on the skin covered by a diaper is quite common. It is usually caused by irritation of the skin from being in contact with stool and urine. It can get worse during bouts of diarrhea.
Diaper rash usually can be prevented by frequent diaper changes.
Jaundice
Jaundice can cause an infant’s skin, eyes, and mouth to turn a yellowish color. The yellow color is caused by a buildup of bilirubin, a substance that is produced in the body during the normal process of breaking down old red blood cells and forming new ones.
Normally the liver removes bilirubin from the body. But, for many infants, in the first few days after birth, the liver is not yet working at its full power. As a result, the level of bilirubin in the blood gets too high, causing the infant’s color to become slightly yellow—this is jaundice.
Although jaundice is common and usually not serious, in some cases, high levels of bilirubin could cause brain injury. All infants with jaundice need to be seen by a health care provider. Many infants need no treatment. Their livers start to catch up quickly and begin to remove bilirubin normally, usually within a few days after birth. For some infants, health care providers prescribe phototherapy—a treatment using a special lamp—to help break down the bilirubin in their bodies.[5]

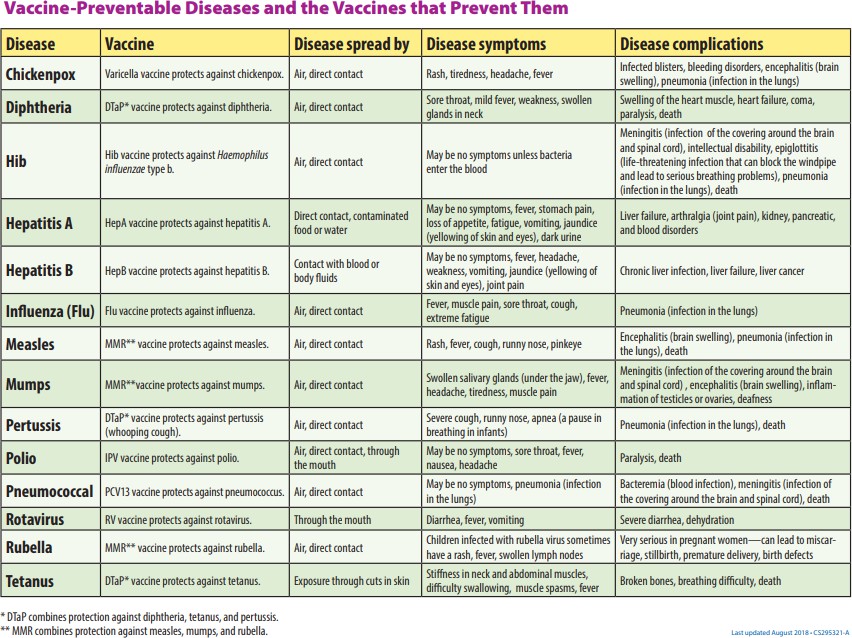
Protecting Health through Immunization
One way we can protect a child’s health (and those around them) is through immunization. The vaccines (given through injection) may hurt a little…but the diseases they can prevent can hurt a lot more! Immunization shots, or vaccinations, are essential. They protect against things like measles, mumps, rubella, hepatitis B, polio, diphtheria, tetanus and pertussis (whooping cough). Immunizations are important for adults as well as for children. Here’s why.
The immune system helps the human body fight germs by producing substances to combat them. Once it does, the immune system “remembers” the germ and can fight it again. Vaccines contain germs that have been killed or weakened. When given to a healthy person, the vaccine triggers the immune system to respond and thus build immunity.
Before vaccines, people became immune only by actually getting a disease and surviving it. Immunizations are an easier and less risky way to become immune.
Vaccines are the best defense we have against serious, preventable, and sometimes deadly contagious diseases. Vaccines are some of the safest medical products available, but like any other medical product, there may be risks. Accurate information about the value of vaccines as well as their possible side effects helps people to make informed decisions about vaccination.

Potential Side Effects
Vaccines, like all medical products, may cause side effects in some people. Most of these side effects are minor, such as redness or swelling at the injection site. Read further to learn about possible side effects from vaccines.
Any vaccine can cause side effects. For the most part these are minor (for example, a sore arm or low-grade fever) and go away within a few days.[6] Serious side effects after vaccination, such as severe allergic reaction, are very rare.[7]
Remember, vaccines are continually monitored for safety, and like any medication, vaccines can cause side effects. However, a decision not to immunize a child also involves risk and could put the child and others who come into contact with him or her at risk of contracting a potentially deadly disease.
How Well Do Vaccines Work?
Vaccines work really well. No medicine is perfect, of course, but most childhood vaccines produce immunity about 90–100% of the time.
What about the argument made by some people that vaccines don’t work that well . . . that diseases would be going away on their own because of better hygiene or sanitation, even if there were no vaccines?
That simply isn’t true. Certainly better hygiene and sanitation can help prevent the spread of disease, but the germs that cause disease will still be around, and as long as they are they will continue to make people sick.
All vaccines must be licensed (approved) by the Food and Drug Administration (FDA) before being used in the United States, and a vaccine must go through extensive testing to show that it works and that it is safe before the FDA will approve it. Among these tests are clinical trials, which compare groups of people who get a vaccine with groups of people who get a control. A vaccine is approved only if FDA makes the determination that it is safe and effective for its intended use.
If you look at the history of any vaccine-preventable disease, you will virtually always see that the number of cases of disease starts to drop when a vaccine is licensed. Vaccines are the most effective tool we have to prevent infectious diseases.
Opposition to Vaccines
In 2010, a pertussis (whooping cough) outbreak in California sickened 9,143 people and resulted in 10 infant deaths: the worst outbreak in 63 years (Centers for Disease Control 2011b). Researchers, suspecting that the primary cause of the outbreak was the waning strength of pertussis vaccines in older children, recommended a booster vaccination for 11–12- year-olds and also for pregnant women (Zacharyczuk 2011). Pertussis is most serious for babies; one in five needs to be hospitalized, and since they are too young for the vaccine themselves, it is crucial that people around them be immunized (Centers for Disease Control 2011b). Several states, including California, have been requiring the pertussis booster for older children in recent years with the hope of staving off another outbreak.
But what about people who do not want their children to have this vaccine, or any other? That question is at the heart of a debate that has been simmering for years. Vaccines are biological preparations that improve immunity against a certain disease. Vaccines have contributed to the eradication and weakening of numerous infectious diseases, including smallpox, polio, mumps, chicken pox, and meningitis.

However, many people express concern about potential negative side effects from vaccines. These concerns range from fears about overloading the child’s immune system to controversial reports about devastating side effects of the vaccines.[8]
Although children continue to get several vaccines up to their second birthday, these vaccines do not overload the immune system. Every day, an infant’s healthy immune system successfully fights off thousands of antigens – the parts of germs that cause their immune system to respond. Even if your child receives several vaccines in one day, vaccines contain only a tiny amount of antigens compared to the antigens your baby encounters every day.
This is the case even if your child receives combination vaccines. Combination vaccines take two or more vaccines that could be given individually and put them into one shot. Children get the same protection as they do from individual vaccines given separately—but with fewer shots.[9]
One misapprehension is that the vaccine itself might cause the disease it is supposed to be immunizing against.[10]
Vaccines help develop immunity by imitating an infection, but this “imitation” infection does not cause illness. Instead it causes the immune system to develop the same response as it does to a real infection so the body can recognize and fight the vaccine- preventable disease in the future. Sometimes, after getting a vaccine, the imitation infection can cause minor symptoms, such as fever. Such minor symptoms are normal and should be expected as the body builds immunity.[11]
Another commonly circulated concern is that vaccinations, specifically the MMR vaccine (MMR stands for measles, mumps, and rubella), are linked to autism. The autism connection has been particularly controversial. In 1998, a British physician named Andrew Wakefield published astudy in Great Britain’s Lancet magazine that linked the MMR vaccine to autism. The report received a lot of media attention, resulting in British immunization rates decreasing from 91 percent in 1997 to almost 80 percent by 2003, accompanied by a subsequent rise in measles cases (Devlin 2008). A prolonged investigation by the British Medical Journal proved that not only was the link in the study nonexistent, but that Dr. Wakefield had falsified data in order to support his claims (CNN 2011). Dr. Wakefield was discredited and stripped of his license, but the doubt still lingers in many parents’ minds.[12]
In the United States, many parents still believe in the now discredited MMR-autism link and refuse to vaccinate their children. Other parents choose not to vaccinate for various reasons like religious or health beliefs. In one instance, a boy whose parents opted not to vaccinate returned home to the U.S. after a trip abroad; no one yet knew he was infected with measles.
The boy exposed 839 people to the disease and caused 11 additional cases of measles, all in other unvaccinated children, including one infant who had to be hospitalized.

According to a study published in Pediatrics (2010), the outbreak cost the public sector $10,376 per diagnosed case. The study further showed that the intentional non-vaccination of those infected occurred in students from private schools, public charter schools, and public schools in upper-socioeconomic areas (Sugerman et al. 2010).[13]
The Immunization Schedule
On-time vaccination throughout childhood is essential because it helps provide immunity before children are exposed to potentially life-threatening diseases. Vaccines are tested to ensure that they are safe and effective for children to receive at the recommended ages.8 Fully vaccinated children in the U.S. are protected against sixteen potentially harmful diseases. Vaccine-preventable diseases can be very serious, may require hospitalization, or even be deadly — especially in infants and young children.[14]
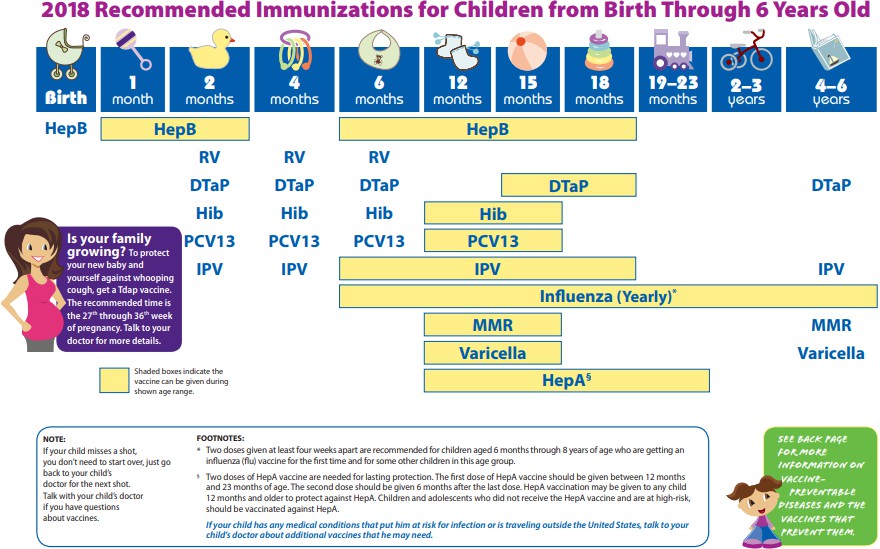
Here is the schedule from the CDC to ensure a child is fully vaccinated:
In this video, Dr. Boise reviews physical conditions and issues during infancy and briefly discusses immunizations.
Safety
There are different risks to infant safety. According to the CDC, nonfatal injury rates varied by age group.
- Nonfatal suffocation rates were highest for those less than 1 year of age.
- Rates for fires or burns, and drowning were highest for children 4 years and younger.
- Children 1 to 4 years of age had the highest rates of nonfatal falls and poisoning.
And the leading causes of injury death also differed by age group.
- For children less than 1 year of age, two–thirds of injury deaths were due to suffocation.
- Drowning was the leading cause of injury or death for those 1 to 4 years of age.[15]
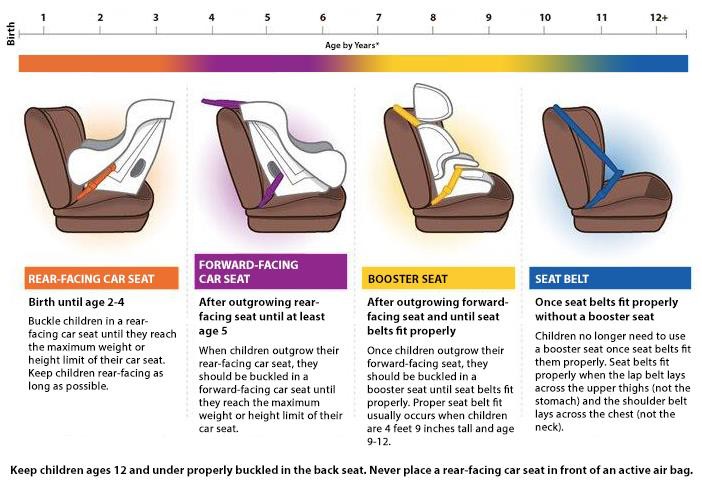
Car Seat Safety
Motor vehicle injuries are a leading cause of death among children in the United States. But many of these deaths can be prevented.
- In the United States, 723 children ages 12 years and younger died as occupants in motor vehicle crashes during 2016, and more than 128,000 were injured in 2016.
- One CDC study found that, in one year, more than 618,000 children ages 0-12 rode in vehicles without the use of a child safety seat or booster seat or a seat belt at least some of the time.
- Of the children ages 12 years and younger who died in a crash in 2016 (for which restraint use was known), 35% were not buckled up.
Buckling children in age- and size-appropriate car seats, booster seats, and seat belts reduces the risk of serious and fatal injuries:
- Car seat use reduces the risk for injury in a crash by 71-82% for children when compared to seat belt use alone.
- Booster seat use reduces the risk for serious injury by 45% for children aged 4–8 years when compared with seat belt use alone.
- For older children and adults, seat belt use reduces the risk for death and serious injury by approximately half.[16]
- Child Growth and Development by Jennifer Paris, Antoinette Ricardo, & Dawn Rymond ↵
- Coping with Crying 3 PSA by the CDC is in the public domain ↵
- Shaken Baby Syndrome by the CDC is in the public domain (modified by Courtney Boise) ↵
- Preventing Abusive Head Trauma in Children by the CDC is in the public domain ↵
- Child Growth and Development by Jennifer Paris, Antoinette Ricardo, & Dawn Rymond ↵
- Disease Prevention and Healthy Lifestyles references Contemporary Health Issues by Judy Baker, Ph.D., licensed under CC BY-SA 4.0 ↵
- Making the Vaccine Decision by the CDC is in the public domain ↵
- Disease Prevention and Healthy Lifestyles references Contemporary Health Issues by Judy Baker, Ph.D., licensed under CC BY-SA 4.0 ↵
- Making the Vaccine Decision by the CDC is in the public domain ↵
- Disease Prevention and Healthy Lifestyles references Contemporary Health Issues by Judy Baker, Ph.D., licensed under CC BY-SA 4.0 ↵
- Making the Vaccine Decision by the CDC is in the public domain ↵
- Making the Vaccine Decision by the CDC is in the public domain ↵
- Disease Prevention and Healthy Lifestyles references Contemporary Health Issues by Judy Baker, Ph.D., licensed under CC BY-SA 4.0 ↵
- Vaccines for Your Children: Protect Your Child at Every Age by the CDC is in the public domain ↵
- Protect the Ones You Love: Child Injuries are Preventable by the CDC is in the public domain ↵
- Child Passenger Safety: Get the Facts by the CDC is in the public domain ↵

{kind=link}
{kind=link}